Rapid Bronchoscopy for ETT Confirmation
Have you ever intubated a patient, initiated sedation, and then the patient started desatting? The ETCO2 is 35. You listen to lung sounds and they seem quieter on the left. The ETT is only at 23 cm and you swear that you barely went past the cords. You already ordered a stat CXR, but it seems xray is not available from 6 am to 7 am (of course). You're pretty sure the patient's hypoxia is just from atelectasis, pneumonia, or pulmonary edema, but you can't help but have an extremely strong urge to get a CXR absolutely NOW!!!
Certainly you can expedite the CXR, but sometimes that can take 10 or 15 minutes, if the patient is teetering on the edge of stability - confirming your ETT is really important.
You basically have two options to help in these moments: bronchoscopy or ultrasound. You can plug in a disposable bronch and just send it down the airway for 10 seconds and have 100% certainty that the ETT is not only in the airway but also above carina and below cords. If the ETT is indeed below the carina, then you can directly visualize carina as it's withdrawn and also view the balloon and cords on the way out.
I'll go over the details and considerations for rapid bronchoscopy for ETT confirmation in this post. Please see this nice video which goes over the simple procedure.
Rapid bronchoscopy for ETT Confirmation
Procedure equipment
- Bronchoscope and monitor (such as GlideScope monitor + BFLEX scope)
- Lubricating jelly or bronchoscope lube
- Bronch adaptor (optional - not needed if short procedure <30 seconds)
Procedure steps
- Place the bronchoscope adaptor in-line if you're using one
- Lubricate the scope
- Put scope into the top of the ETT or through bronch adaptor
- Advance the scope slowly until you get to the very end of the ETT
- Use your thumb to angle the camera up or down and look for signs that you are in the trachea and for the main carina
- Advance the scope just until the main carina
- Note the depth of the proximal part of the scope with fingers or tape
- Pull the bronchoscope back until it is just at the tip of the ETT
- Estimate the distance from the ETT tip to the carina
- Reposition ETT if needed
Disposable bronchoscopes are cheap
First things first: a disposable bronchoscope cost about 200$ and video glidescopes cost about 75$. Don't let the cost sway you from opening one up. If it's going to be useful for the patient, then just use it.
Bronchoscope sizing
Any scope will fit in a 7-0, 7-5, or 8-0 tube
A smaller scope is better for 7-0 or less
Bronchoscopes sizes are in millimeters and range from 3 mm - 6 mm. The size is always reported as the outer diameter. Ideally, your bronchoscope will be 2 mm smaller than your ETT. As long as the bronchoscope it is 1 mm smaller than the ETT and well lubricated you will be perfectly fine for a simple ETT depth check procedure.
So, for example, any bronchoscope could be used for an 8-0 or 7-5 tube comfortably. The larger bronchoscopes, often called the "therapeutic scope," are typically 5.8 mm and would work ok for a 7-0 tube, but it would be tight. A therapeutic scope CERTAINLY would NOT work for a 6-0 or 6-5 tube.
These are the current versions of the GlideScope BFLEX 2 disposable flexible bronchoscopes.

Bronch adaptors
When you're first learning how to do this, you should use a bronchoscope adaptor. Sometimes this is called a bronch swivel. You put this on the end of the ETT like an in-line suction device. It has a small opening that you can place the bronch through. This lets you oxygenate and ventilate while doing the bronchoscopy.


Ventilator Alarms and Settings
Placing the bronchoscope in the ETT through an adaptor increases the resistance of the system a lot, so on the ventilator you should expect the peak pressures to be super high (volume control) or tidal volumes to be super low (pressure control). Experienced respiratory therapists will automatically increase the alarm and put the patient on volume control. This increased peak pressure represents resistance in the system NOT in the patient - so do not worry about it.
If you're just doing a quick in/out bronch to confirm the ETT, you don't really need to change the vent mode at all. If you plan to take more than a minute, you should be on volume control and avoid pressure control, pressure support, or PRVC.
Lubricating the Bronchoscope
If the ETT is quite large and your scope is small you are definitely ok using an unlubricated scope. For example, an 8-0 tube should allow any scope down without lubrication. If you have a moment, lubrication makes the procedure quite a bit easier.
You only need to lube up the second half of the scope since most of it will be outside of the ETT.
You can use just standard normal lubricating jelly.
In most places, your respiratory therapist will know where to find the bronchoscope specific lubricating jelly. This stuff lasts a little bit longer and is a little more slippery. It's fine to just use normal lube if you can't find the special stuff.


Identifying the trachea
The following structures can look surprisingly similar - especially in a high stress situation.
- Trachea + main carina
- Right main bronchus + RUL carina
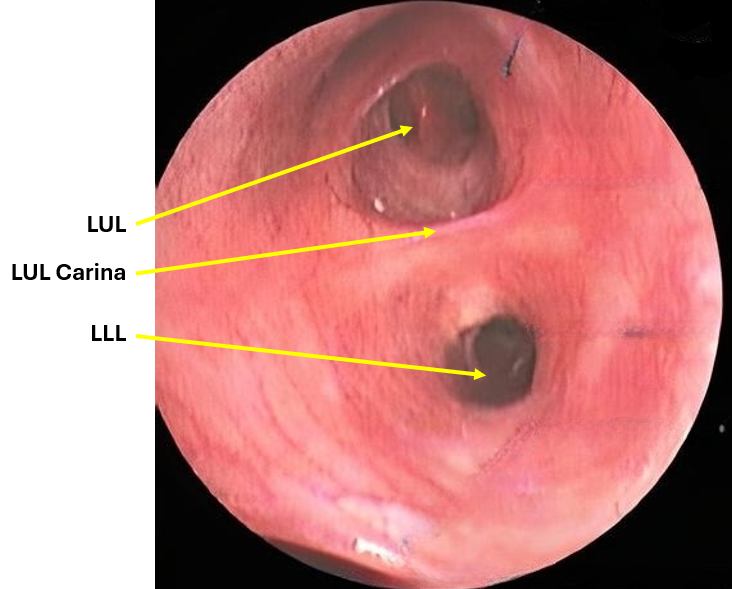
- Left main bronchus + LUL carina
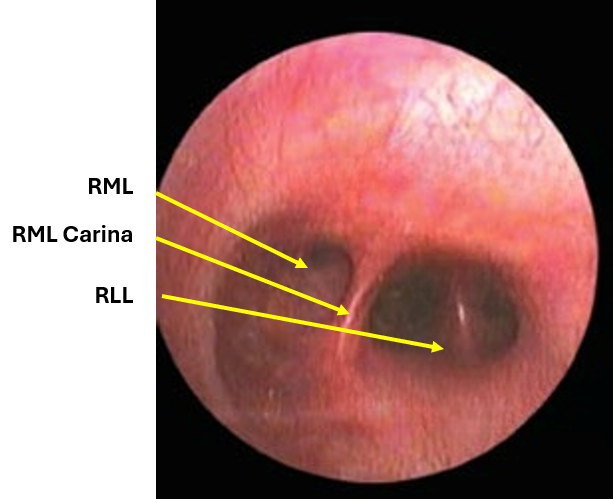
- Bronchus intermedius + RML/RLL carinas
You certainly don't need to be able to name and identify these structures in order to confirm an ETT, but you should recognize that they DO NOT look like the main carina. You want to avoid the situation where you "confirm" an ETT, but because you misidentified one of these as the main carina, you are falsely reassured.
It helps if you advance your scope slowly once you are at the tip of the ETT, so you don't accidentally blast past the main carina.
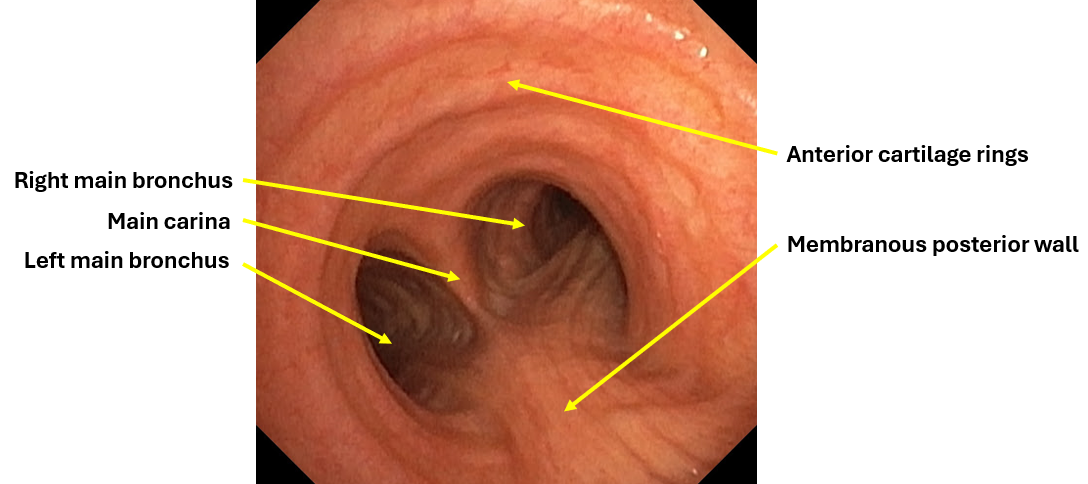
Trachea and main carina
The trachea has a large bore, oval shape, anterior cartilaginous rings, and a membranous posterior wall.
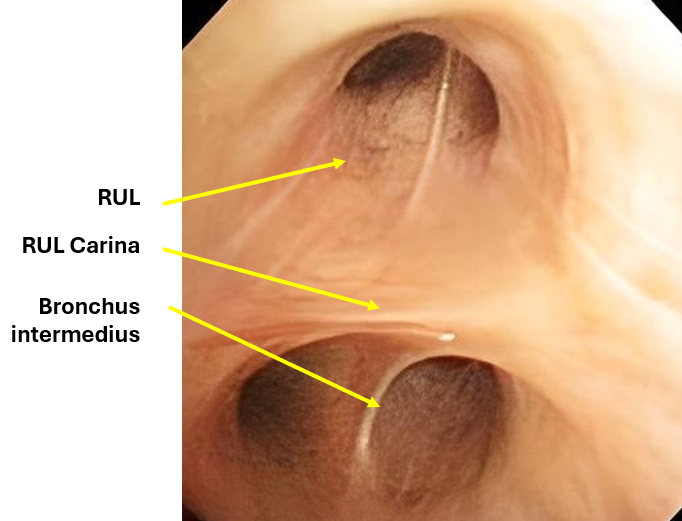
Right main bronchus + RUL carina
Bronchus intermedius + RML/RLL carinas
Left main bronchus + LUL carina
In general, note the lack of oval shape, anterior rings, and posterior membranous wall.
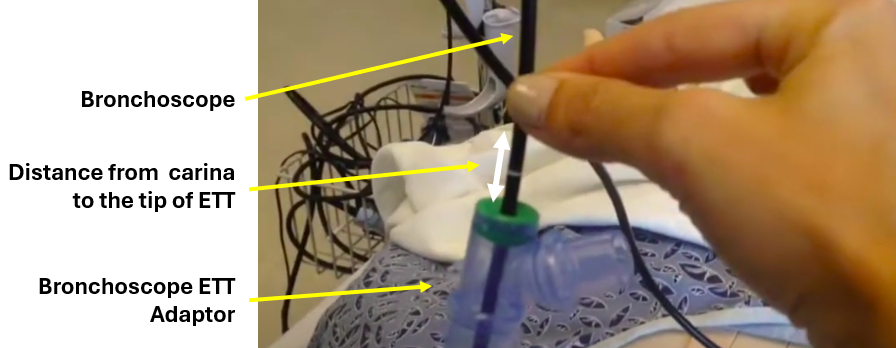
Measuring ETT depth
The idea here is to use the bronchoscope as a measuring stick. You put the bronchoscope at the main carina, and pull it back just to the tip of the ETT. However much you pulled the bronchoscope out is the distance from the carina to the tip of the ETT. This is quite easy: get the scope to the carina, have an assistant pinch the scope just as it enters the ETT or the bronchoscope adaptor, and then pull the scope back to the tip of the ETT. Estimate the distance from the assistant's fingers to where the ETT or adapter.
Summary
Bronchoscopy can be an indispensable tool when you're worried about the location and depth of an ETT.
Sometimes CXR takes way longer than you ever imagined was possible and you need to lean on this complementary airway confirmation tool.
Rapid bronchoscopy for ETT confirmation is a safe and simple method to both confirm your ETT depth and also correct it if you are too deep.