Advanced Vascular Access Techniques for the Intensivist
The intensivist is a master of vascular access, but from time to time we still find ourselves with a challenging case. Sometimes the odds stack against our favor. Think of an elderly patient who is on dialysis, in shock, obese, and with just a small little femoral artery. When you're going 6 cm down to a tiny little calcified femoral artery it can be difficult.
This article exists to discuss some tips, tricks, and advanced concepts for these difficult cases.
Know your units and equipment
- 1 Fr = 1/3 mm
- Gauge conversions are not strictly defined. Use the following table as a reference for inner/outer diameter of IV catheters
| Gauge | Colour | ID - OD (mm) |
|---|---|---|
| 14 | Orange | 1.6-2.1 |
| 16 | Grey | 1.3-1.7 |
| 17 | White | 1.2-1.5 |
| 18 | Green | 0.9-1.3 |
| 18 | Green | 0.9-1.3 |
| 20 | Pink | 0.8-1.1 |
| 22 | Blue | 0.6-0.9 |
| 24 | Yellow | 0.5-0.7 |
| 26 | Violet | 0.4-0.6 |
Use a micro-puncture kit
All hospitals have micro-puncture kits which include a needle, wire, and introducer. There are many things about the kit that make it special and advantageous for difficult access. The kit contains the following items:
- Needle - 21g with 1.0 mm OD and 0.7 mm ID
- Wire - 26g with 0.018" or 0.5 mm diameter
- Introducer - 4 Fr (1.3 mm) or 5 Fr (1.7 mm)
For comparison, a typical central line kit has a 18g, 1.3 mm OD, needle and a 0.035" (0.9 mm) wire. The numbers are small, but really, the 18g needle is quite a bit bigger than the micro-puncture needle.
The advantage of a smaller needle is that it cuts through tissue easier, is less likely to damage the artery, and less likely to cause a hematoma. Furthermore, the needle is specially designed to be echogenic on the anterior (bevel up) surface.
The smaller needle enters a vessel with less force, so it is much easier to enter a very compressible or calcified vessel.
The wire is special as well. When a J tip wire comes out of the needle, it immediately curls prior to advancing. The idea is to prevent injury to the vessel. The problem is that if you're coming in from a steep angle or the vessel is small, then the J tip cannot make the turn out of the needle to go up the vessel. The micro-puncture wire is small and also has a soft, flexible, and straight tip, so when it comes out of the needle it is more likely to be able to navigate the area between the needle tip and the vessel instead of just pushing into the posterior wall.
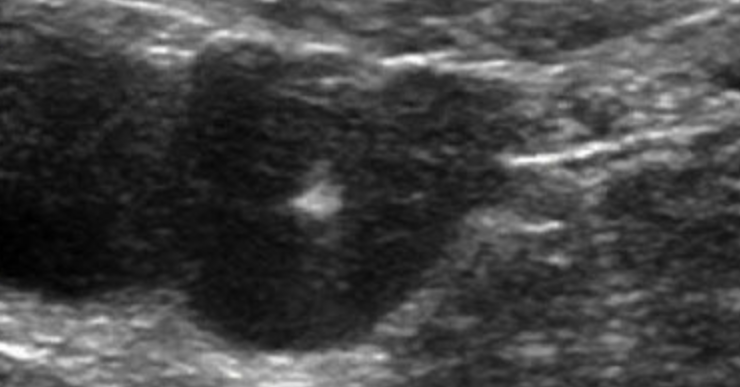
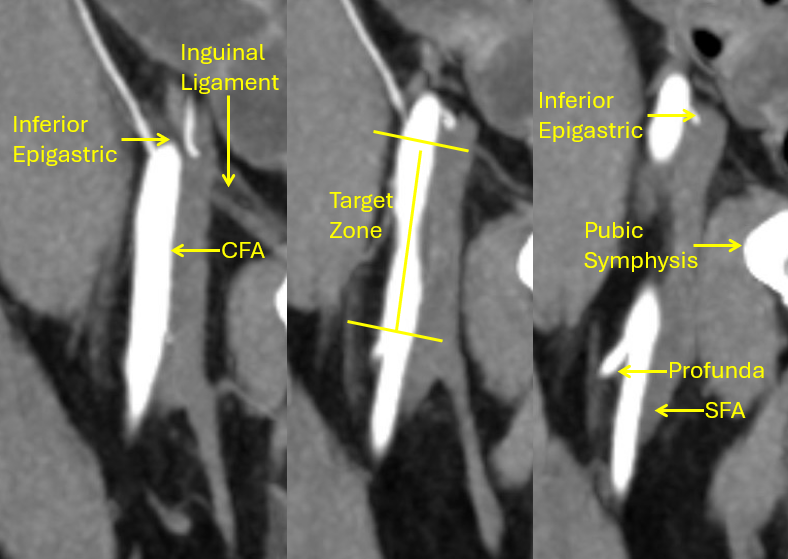
Know how to find COMMON femoral
Before even evaluating the patient, you need to review any available cross sectional imaging - assuming you have the time. This will help you know going in about the anatomy of the inguinal ligament and femoral vessels. In particular, sometimes the common femoral artery branches into profunda and superficial femoral artery more superior on one side. So it's advantageous to take a look ahead of time if you anticipate a difficult line.
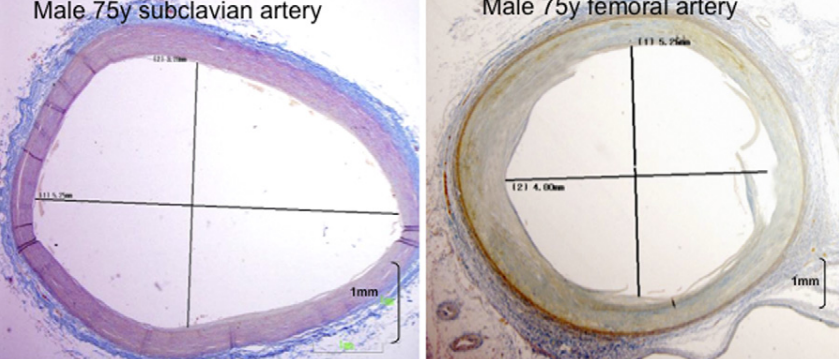
Consider using the axillary artery
Femoral access can be unfavorable due to low caliber, depth, or severe PAD. The axillary vein and artery are only about 10% smaller than the femoral vein and artery. They are large enough to be used for ECMO, IABPs, or Impella devices so they are definitely big enough for your arterial line. Furthermore, as long as you stay lateral, you most certainly remain away from the lung and in a compressible site.
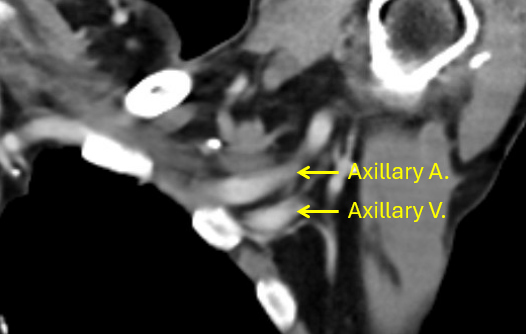
Avoid the brachial plexus
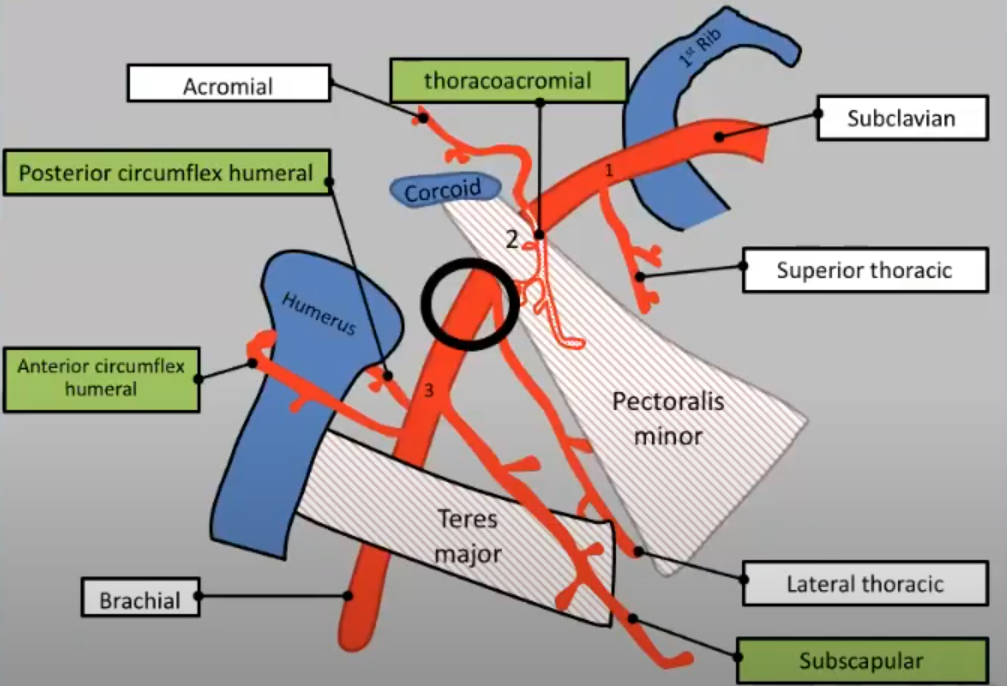
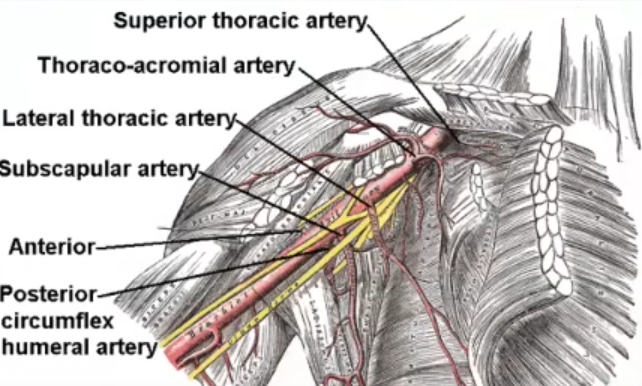
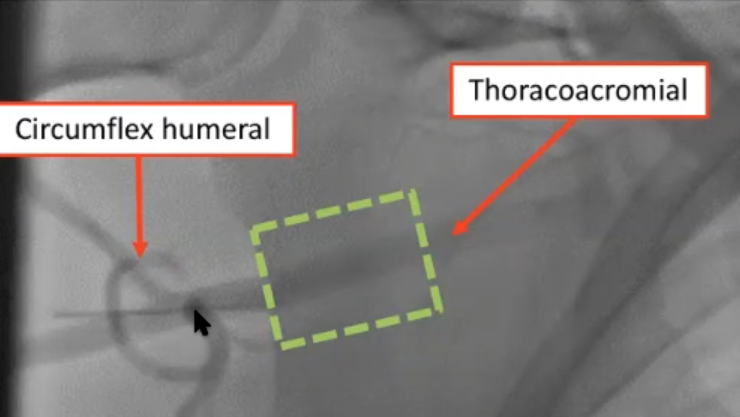
The main thing to be thoughtful about for axillary lines is to avoid the brachial plexus. You want to access the artery in the second portion defined between the thoraco-acromial artery and the subscapular/circumflex humeral artery. The pectoral minor muscle goes over this, so you'll certainly have to go through it.
Consider avoiding left axillary if the patient has a history of CABG with LIMA graft.
You want to be above the circumflex humeral in case there is an arterial injury and it needs to be stented.
Summary
- Practice with micro-puncture kits
- Know your femoral anatomy
- Know how to safety access the axillary artery