CRRT - lost in the sauce

The hardest part about learning CRRT is deciphering the alphabet soup. It's easy to get lost in the sauce.
Once you learn concretely the vocabulary and what all the tubes and pumps do on the CRRT machine then the rest kind of just falls in to place.
This article is targeting physicians at the senior resident or early fellow level looking to really understand the different kinds of CRRT, how to manage them, and how to troubleshoot issues.
I assume almost no prior knowledge.
Banned vocabulary
To start off with, let's just go ahead and ban a bunch of words for a little while. They have meaning and are useful, but right now it's just semantics.
- Anything that starts with Q, C, FF, TMP, or K
- Clearance
- Convection
- Diffusion
- Filtration fraction
- Sieving coefficient
- Effluent
- SOLVENT
- SOLUTE
- Ultrafiltrate
- CVVHD
- CVVHDF
- CVVH
- SLED
- SCUF
CONCRETE and FUNDAMENTAL
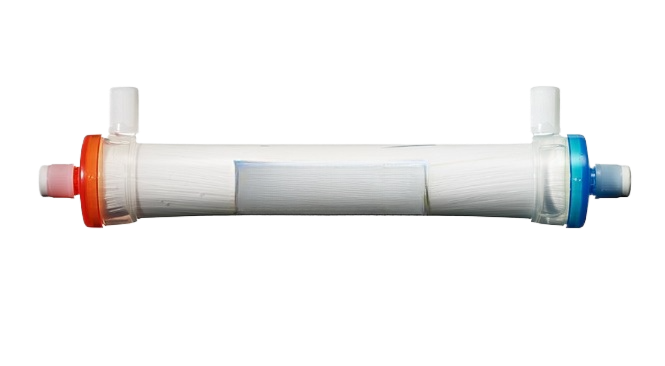
This is a filter
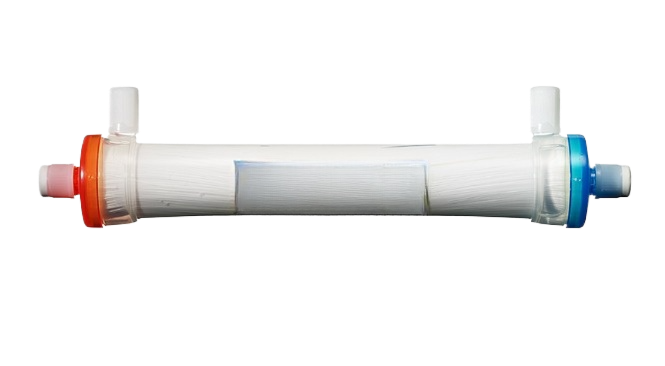
A filter has FOUR places that tubing can be connected.
Blood goes in the red end and out the blue end.
Filtered fluid comes OUT the red side port. It is hooked up to a PUMP which can remove fluid at a set rate.
Fluid CAN be infused into the blue side port BUT sometimes we don't use this one. It depends on they type of CRRT.
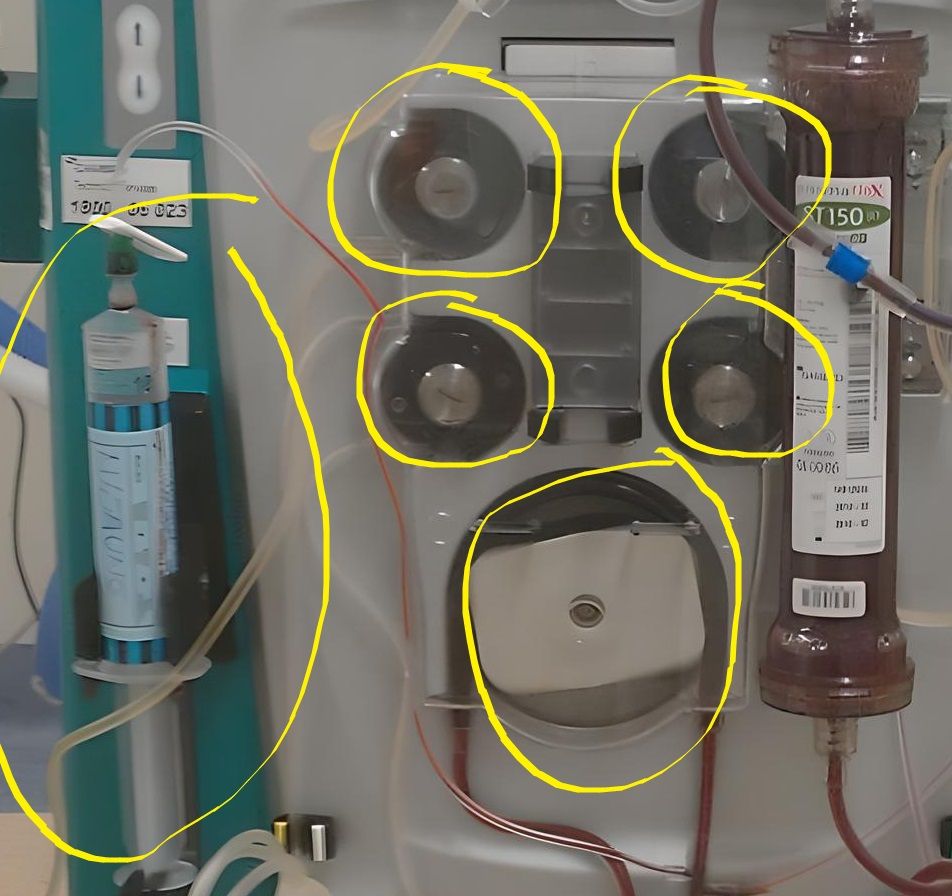
This is a CRRT machine
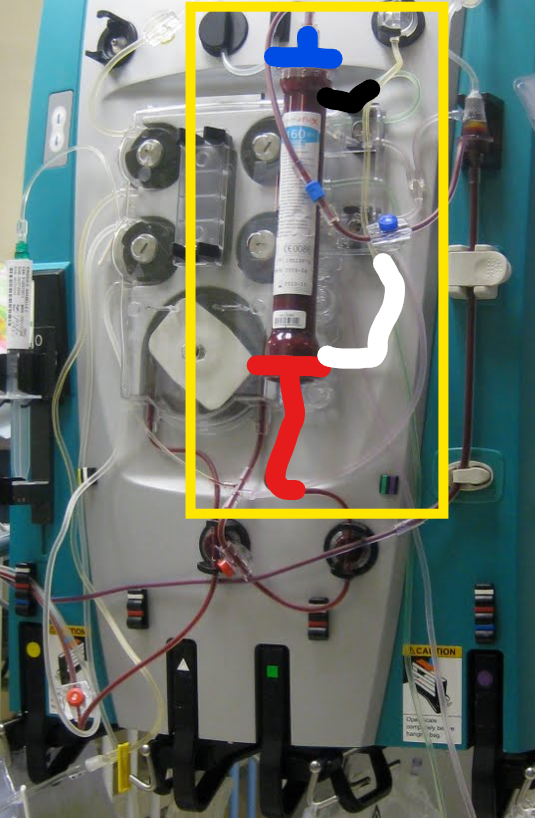
Blood goes in the red end and out the blue end.
Filtered fluid comes out the white port (it's rotated and actually behind the filter). THIS IS CONNECTED TO A PUMP THAT CAN PULL FLUID OUT.
Dialysis fluid can sometimes go in the black port - depending on CRRT mode.
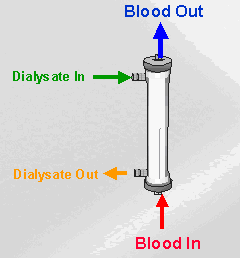
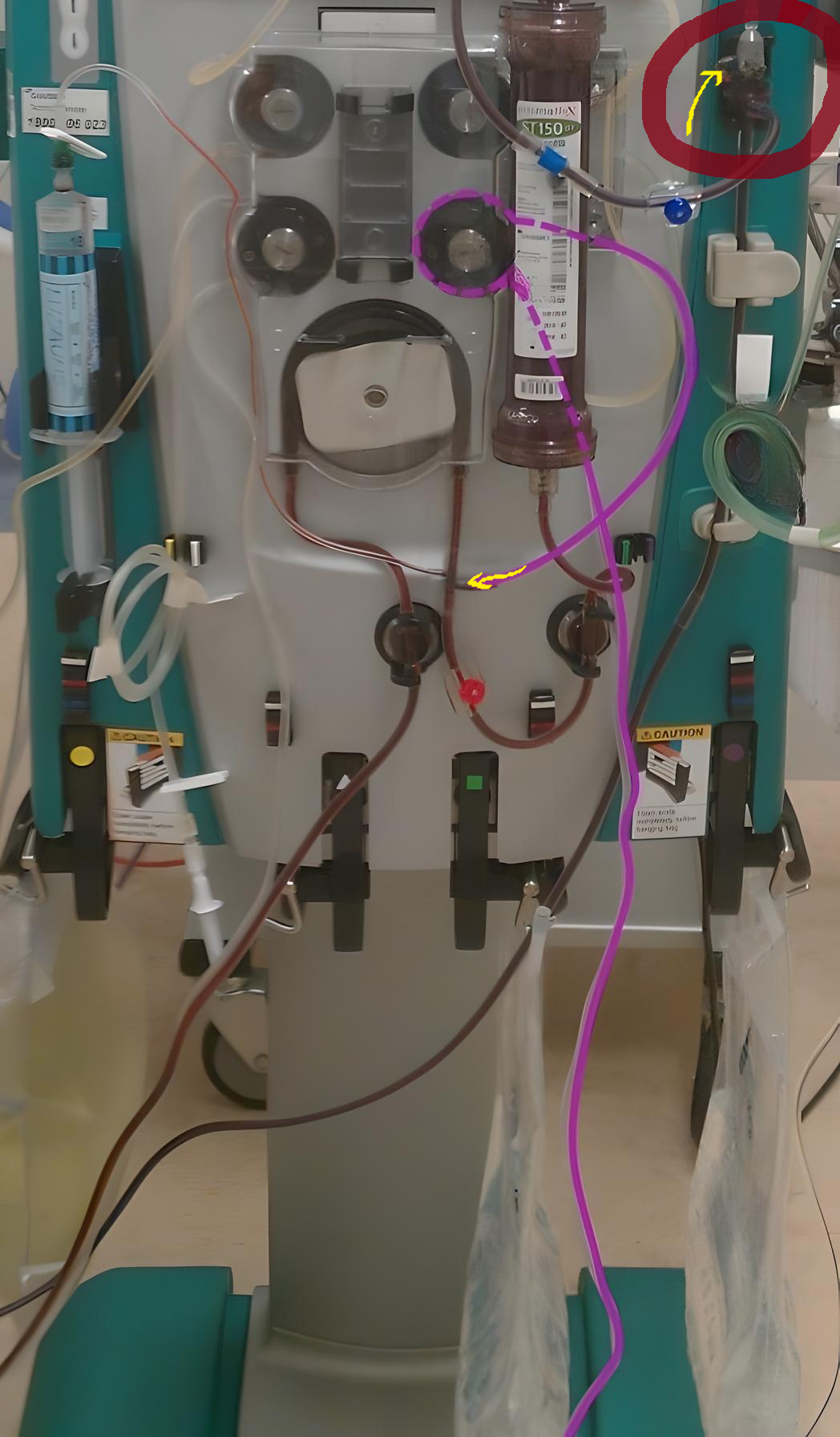
This is a CRRT machine on it's side
Maybe this is getting redundant, but blood GOES IN THE RED PORT and OUT THE BLUE PORT. Filtered fluid comes OUT the white port to a PUMP and fluid CAN SOMETIMES go in the black port.

Nobody talks about all the pumps!
You know an IV pump, it pumps stuff?
Well, CRRT pumps also pump stuff.
THERE ARE LITERALLY 6 PUMPS ON THIS THING
Each pump can create a negative pressure from whatever it's pulling on.
Each pump can create a positive pressure on whatever it's pushing on.
There are lots of measured pressures on the CRRT machine, some are negative and some are positive.
There is no guess work in CRRT, all of the flow rates are finely tuned and controlled.
When blood goes through the FILTER it gets FILTERED
The membrane has holes in it and fluid leaks out. The fluid that leaks out has molecules from the plasma in it. THINGS LIKE UREA, FOR EXAMPLE.
In fact, for really small molecules (LIKE UREA), the concentration in the fluid that leaks out is MAGICALLY about the SAME as that in the plasma or blood!
If all we did was run blood through a FILTER and COLLECTED the leaky fluid we call it SCUF
Slow Continuous Ultrafiltration is abbreviated SCUF, but I'll continue to spell it out because of the alphabet soup situation.
It's called SLOW because it doesn't remove bad molecules very fast. Only the fluid that leaks out has things like urea in it. You can only collect a little bit at a time because every drip/drop is removed from the patient's circulating volume. If it was FAST continuous ultrafiltration, then the patient would get hypotensive and die.
It's CONTINUOUS (duh).
ULTRAFILTRATION just means filtration. I don't know why it's ultra. "ULTRAFILTRATE" it's basically just the equivalent of the fluid that leaks out during slow continuous ultrafiltration.
Slow continuous ultrafiltration is VERY bad at removing bad things from the blood (like potassium or UREA FOR EXAMPLE). The ONLY thing SCUF is good for is to remove FLUID from the patient. It does NOT remove bad molecules very well.
WELL... if we can't collect TONS of the fluid that leaked out of the filter SLOWLY, then LETS GO FAST and just replace it with clean plasma?!!
This is called CONTINUOUS VENO-VENOUS HEMOFILTRATION (CVVH).
I swear it's all in the name: Continuous. Venous to venous. Filters heme (blood).
In slow continuous ultrafiltration (SCUF), we can only collect a little bit of the fluid that leaks out when blood goes through the filter. We can go ahead and collect a LOT more if we just give the patient back some clean plasma.
THE "CLEAN PLASMA" IS CALLED REPLACEMENT FLUID
In real life, in the Americas at least, this is usually the fancy brand name fluid called Prismate. It just has some isotonic combination of water, sodium, chloride, bicarbonate, calcium, and magnesium. It's literally just a small variation compared to Lactated Ringers, Plasmalyte, or "normal" saline.
So we just take out the bad fluid and replace it with good fluid - easy!
SO THEN: HOW MUCH REPLACEMENT FLUID SHOULD YOU USE?
If you know, you know. This question is SUPER LOADED.
We basically need to remove enough of the leaky fluid to get rid of all the patient's bad stuff. I mentioned that the concentration of bad stuff in the leaky fluid is roughly similar to it's concentration in plasma for small molecules like UREA and POTASSIUM - for example. So we basically just take off as much fluid as we need to get rid of all the bad stuff and give enough of the good fluid back to match the volume.
IT'S WAY MORE THAN YOU THOUGHT
The short answer to this loaded question is that you need to remove 25-35 ml/kg/h of the leaky fluid.
YEP, LIKE 2 LITERS PER HOUR (48 LITERS PER DAY)
Since the patient would DEFINITELY die if you pulled off 2 liters per hour, we just give them back clean plasma (replacement fluid) to REPLACE what we took.
YOU JUST TAKE OUT ALL THE BAD HUMORS AND REPLACE THEM WITH GOOD HUMORS
OK, SO WHICH PORT DOES THE REPLACEMENT FLUID GO IN!?
Psyche. NONE OF THEM. It just get's Y'd in somewhere in the tubing.
In fact, you can put the replacement fluid either BEFORE or AFTER the filter.
If you put it BEFORE the filter, then it helps prevent the filter from clotting, but it dilutes out the molecules in the leaky fluid - so you end up having to take a bit more volume AND replacing a bit more volume.
If you put it AFTER the filter, then your leaky fluid is more concentrated with bad stuff, so you don't have to take AND replace quite as much volume BUT your filter might just clot right off.
Should I put the fluid BEFORE or AFTER the filter?
It depends on what you're trying to achieve with the CRRT. If you're trying to get as much bad stuff out as possible, then after is better so long as the filter isn't clotting off.
If your filter is clotting off, then you can put it before
Why not both?
This is ALSO a loaded question.
Yes, you can do some portion of fluid BEFORE and some portion AFTER. For example, you can do 70% of the fluid AFTER the filter and 30% of the BEFORE the filter.
So, for a 60kg person this may look something like:
- Remove 25 ml/kg/hr of leaky fluid with the bad stuff in it
- 25 ml/kg/hr * 60 kg = 1500 ml/hr
- So, remove 1500 mL per hour of BAD fluid
- Give 500 mL per hour of good fluid BEFORE the filter
- Give 1000 mL/hour of good fluid AFTER the filter
*good fluid = replacement fluid :)
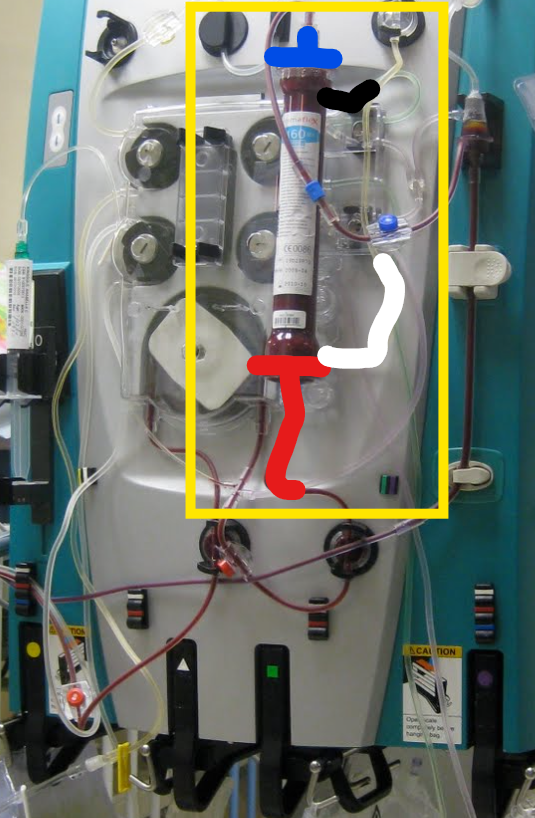
Why are all these tubes so hard to see in pictures?!
This patient is only hooked up to PRE FILTER replacement fluid. You can see that the fluid is literally just Y'd into the tubing just before the BAD BLOOD goes INTO the RED PORT of the filter.
For the POST filter replacement fluid, it actually just connects at the red circle/yellow arrow on that little thingamajig there. Yes, this is a technical name for an air bubble remover. It doubles as the place where you Y in the replacement fluid.
Are we even doing dialysis yet?
Well, not really...
Up until now we've just been doing hemoFILTRATION.
NOW we're going to talk about hemoDIALYSIS
What exactly is dialysis!?
Remember in biology when you had a semi-permeable membrane and you put a fluid on one side and it just stayed there, but another fluid just went right through?
That's dialysis.
There is a concentration gradient and a molecule that can go through a semi-permeable membrane (LIKE UREA FOR EXAMPLE!!!).
So far we've talked about slow continuous hemoFILTRATION and continuous veno-venous hemoFILTRATION but at NO POINT have we separated two fluids with different concentrations of stuff with a semi-permeable membrane.
OK, let's do continuous veno-venous hemoDIALYSIS!
This is abbreviated CVVHD.
OK now we're really getting into the alphabet soup (sauce?)
TO SUMMARIZE:
- SCUF is slow continuous hemoFILTRATION
- CVVH is continuous veno-venous hemoFILTRATION
- CVVHD is continuous veno-venous hemoDIALYSIS
Remember the blue side port? This is how you do dialysis!
Blood goes IN THE RED PORT and OUT THE BLUE PORT
Dialysis fluid goes IN the BLUE SIDE PORT and OUT the RED SIDE PORT
Dialysis fluid literally the same kind of fluid as replacement fluid
So the fluid that goes in the blue side port is like "clean plasma"
Since blood has bad molecules in it and the "clean plasma" (dialysate) doesn't have bad molecules in it. NOW we have a concentration gradient between the two fluids and they're separated by a semi-permeable membrane (aka the filter).
Now that this is all set up, all bad molecules in the bad fluid diffuse over in to the good fluid. So if we just keep replacing the dialysate with new "clean" dialysate, then we'll keep removing bad molecules.
The RATE of fluid going into the blue side port roughly EQUALS the rate of the fluid coming out of the RED side port. When we're doing continuous veno-venous hemoDIALYSIS if we USE THE PUMPS to set the dialysate removal rate HIGHER than the dialysate infusion then we'll generate EXTRA BAD FLUID.
Concretely, if we have good dialysate going IN the BLUE SIDE PORT at 1000 ml/hr and bad dialysate coming OUT the RED SIDE PORT at 1200 ml/hr then it would be kind of similar to doing slow continuous hemofiltration (SCUF) with 200 ml/hr of fluid removal. By having these different flow rates, we are able to generate ultrafiltrate which removes a small amount of extra bad stuff and lets us remove volume.
IS DIALYSIS EVEN GOOD AT ANYTHING?
Compared to hemoFILTRATION, hemoDIALYSIS is much better at removing bad molecules from the blood.
I've noticed that all my patients are on CVVHDF
Ok, ok, let's put it all together to get to the mode that is most often used.
Continuous veno-venous hemoDIAFILTRATION (CVVHDF)
To summarize again:
- SCUF is slow continuous hemoFILTRATION
- CVVH is continuous veno-venous hemoFILTRATION
- CVVHD is continuous veno-venous hemoDIALYSIS
WHAT IF WE RAN DIALYSIS
AND ALSO PULLED TONS OF BAD FLUID
AND ALSO GAVE LOTS OF GOOD FLUID?
You can USE THE PUMPS to give/take wherever you want until the filter clots or your venous access gives out.
You can pull the bad fluid from the RED SIDE PORT at a much higher rate than you give dialysate though the BLUE SIDE PORT. But then you have the same situation as in slow continuous ultrafiltration (SCUF) where you're patient would get hypovolemic and die. So, go ahead and give them replacement fluid Y'd in to the tubing somewhere (pre or post filter).
Why use CVVHDF?
The jist of it is that you can get away with lower blood flow rates and still remove all the bad stuff and fluid.
Which is the best mode of CRRT?
Let's talk about Klearance
The time has come. Clearance is a weird value because it's not the AMOUNT of bad stuff removed. It's the volume of bad blood that is converted into good blood in a given time.
Clearance is abbreviated as K.... how Konfusing.
I mentioned a few times that the concentration of a small bad molecule in the blood is almost the same as in the bad fluid coming out of the filter. So if you take out 1500 milliliters of bad fluid in 60 minutes for a 60 kg person, then the clearance of a small molecule is about 25 mL/kg/hr.
Is the clearance different if the BUN is 100 vs 30?
No, in these two scenarios the AMOUNT of urea removed in 1 hour would be different, but the VOLUME of "bad blood" converted into "good blood" is actually the same.
Why should I even care about clearance?
Consider what would happen if you put a patient with ZERO renal function on non-stop CRRT with some stable settings for 2 weeks. What would happen to the blood concentration of the bad stuff like urea?
Well, their body is always making urea, so their blood level would never reach zero, and the CRRT is always removing urea. AHAH THEY REACH A STEEADDDY STATE.
Hair in the drain
I've always enjoyed thinking about steady states like bath tubs.
Input is the faucet. Output is the drain.
If there is some hair in the drain and you put the water on, then the tub will eventually just chill at a low level.
The body makes urea. CRRT removes urea.
If somebody is on CRRT for A LONG TIME then the urea level will reach some steady level. And how high is that level?! Ahh, yes, it depends on the clearance.

You need 25-35 ml/kg/hr of clearance to maintain a normal level of the bad stuff
For a given molecule you want to essentially clear ONE volume of distribution per "dialysis session," CONTINUOUS renal replacement therapy is (*hopefully*) a 24 hour session.
The volume of distribution of urea is total body water, or 60% of the weight.
So for a 60kg person, you want to clear 0.6 L/kg * 60 kg = 36 L PER DAY.
Restated, you need to "clear" 36 liters per day.
So basically K * 24h = 36 L = 1.5 liters
1.5 liters just so happens to be 25 ml/kg/hr for 24 hours :)
ALL THE WORDS I DIDN'T USE BEFORE
WHAT IS ULTRAFILTRATE
Ultrafiltrate is the NET fluid that is filtered out of the blood in ANY mode of dialysis. It's often mixed in with replacement fluid and/or dialysate.
WHAT IS EFFLUENT?
Effluent is EVERYTHING that comes out of the red side port. What it consists of depends on the mode of CRRT.
For this whole post, when I say "leaky fluid" or "bad fluid" I usually really am talking about effluent.
- Slow continuous ultrafiltration (SCUF): effluent is all the filtrate from blood and it equals ultrafiltrate.
- Continuous veno-venous hemofiltration (CVVH): effluent is ultrafiltrate + replacement fluid, irregardless of where your replacement fluid is infusing.
- Continuous veno-venous hemodiafiltration (CVVHD): effluent is dilaysate + replacement fluid + ultrafiltrate.

Sieving coefficient
Small molecules equilibrate in the effluent. Large molecules can't even get through the filter. How well a particular compound can get through the filter pores is defined by the sieving coefficient.